Melasma
Melasma
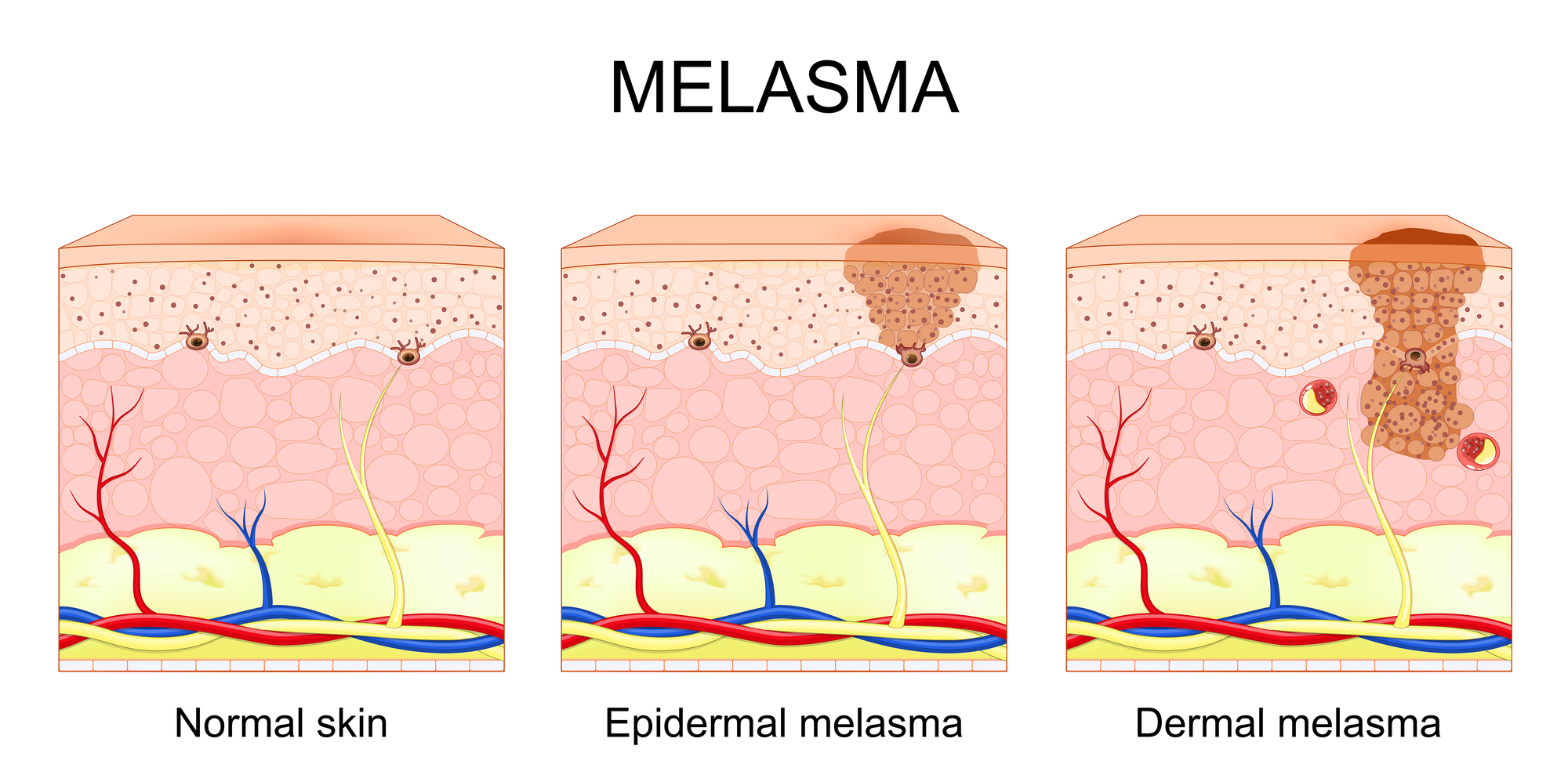
Melasma is a chronic acquired hyperpigmentation disorder characterized by irregular brown to gray-brown facial patches, most commonly affecting the cheeks, forehead, upper lip, and chin. It is influenced by ultraviolet exposure, hormonal factors, inflammation, and genetic predisposition.