Persistent
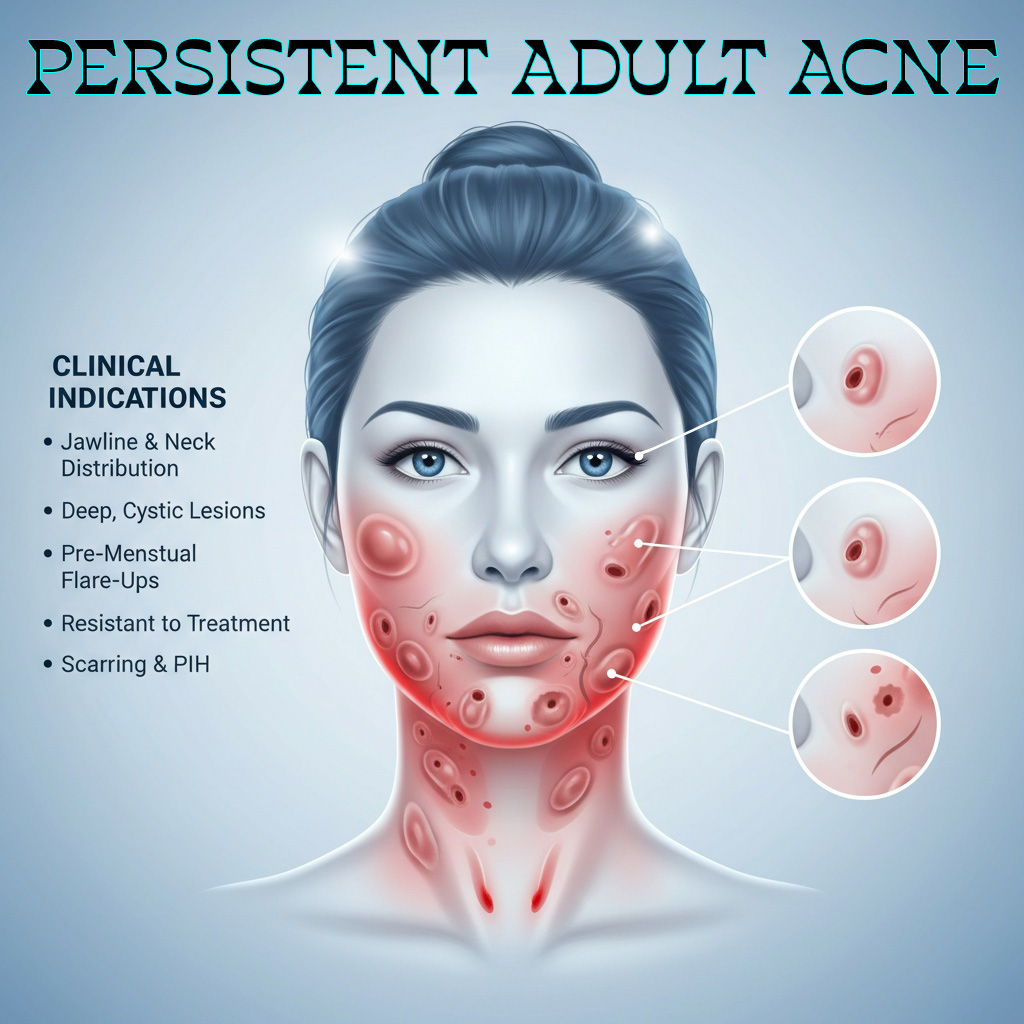
Adult Acne
A chronic inflammatory and metabolic skin disorder requiring more than symptomatic suppression.
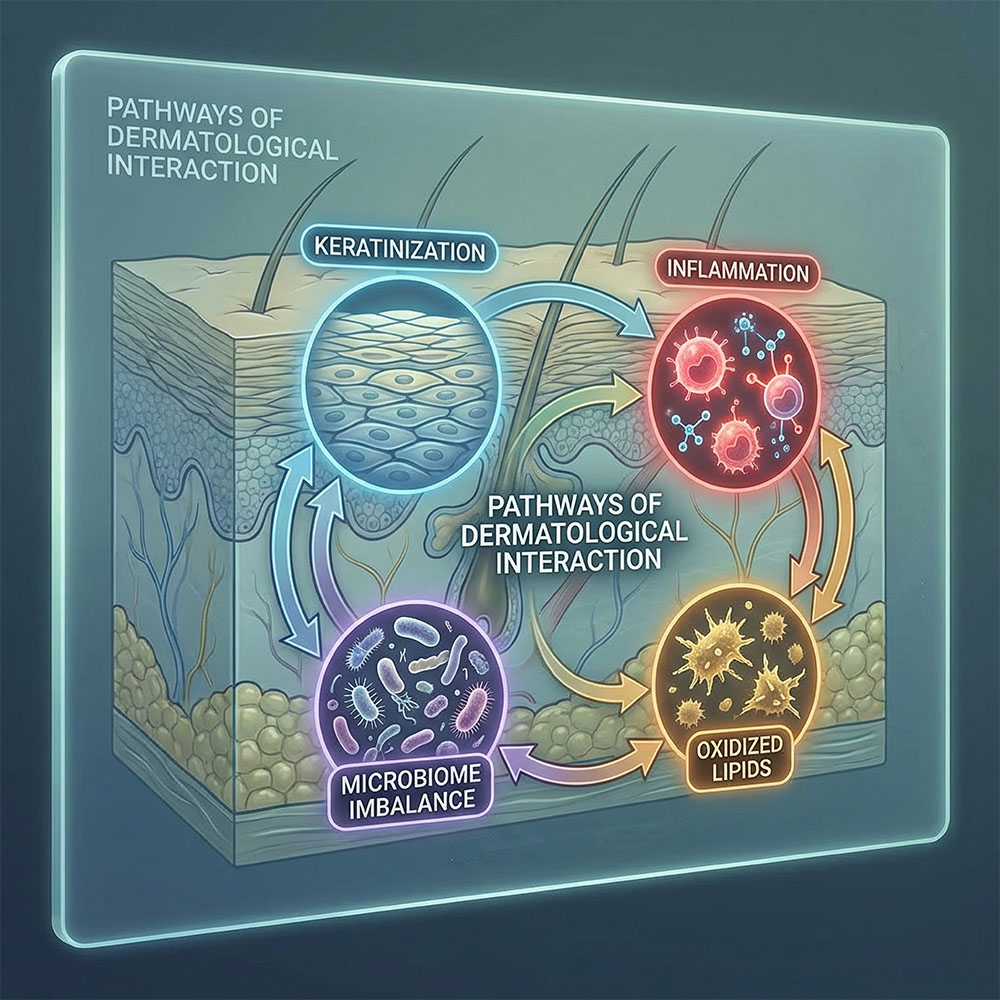
Persistent adult acne is not simply adolescent acne that never disappeared. In many patients, it reflects a more complex biological pattern involving chronic low-grade inflammation, altered follicular regulation, microbiome imbalance, oxidative stress, and impaired epidermal control. The objective is not merely to dry lesions, but to restore skin function with precision.
More persistent, more inflammatory, and often more resistant than conventional acne patterns.
Move from repetitive suppression toward controlled biological regulation and epidermal rebalancing.
Support turnover, reduce inflammatory persistence, and optimize the skin environment without unnecessary aggression.

Adult acne management requires controlled intervention, not repeated irritation. The aim is to reduce lesion persistence while restoring epidermal coherence.