High-Intensity Controlled Chemical Action Not a peel. A controlled chemical intervention.
TCA 30% w/w is a high-strength liquid professional peel designed for advanced protocols requiring precise application, strict control of exposure time, and expert clinical judgment. Its elevated concentration — equivalent to approximately 35% w/v — produces a stronger epidermal response with clearly defined tissue coagulation and intense desquamation.
⚠️ Professional Use Only: This high-strength formulation is intended exclusively for trained practitioners. Incorrect application or excessive exposure may lead to significant tissue injury.
TCA 30% is not designed to replace lower concentrations. It exists to address clinical situations where controlled chemical intensity becomes necessary to trigger a meaningful biological response. It represents a different level of clinical intervention, where precision of application, exposure control, and tissue response management become critical. Its use is justified when superficial approaches are insufficient to achieve meaningful skin remodeling.
Higher Biological Impact
The increased concentration allows a more pronounced epidermal coagulation, leading to a stronger regenerative cascade and visible structural improvement in selected indications.
Precision Over Power
The effectiveness of TCA 30% does not rely solely on its strength, but on controlled application, layer management, and timing. It is a tool of precision rather than brute intensity.
Indication-Driven Use
TCA 30% is reserved for cases where lower concentrations cannot produce sufficient clinical response, including resistant dyschromias, textural irregularities, and advanced epidermal damage.
Clinical outcome depends on practitioner expertise, protocol selection, and patient-specific variables. TCA 30% should be integrated within a structured treatment strategy rather than used as a standalone intensity escalation.
Why TCA 30% Exists as a Liquid Formulation Only
At high trichloroacetic acid concentrations, formulation logic becomes a matter of chemical integrity rather than simple texture preference. TCA 30% is therefore presented as a liquid-only professional peel, consistent with the stability requirements of high-intensity acid protocols and with the need for precise clinical application.
TCA 30% is not a comfort-oriented peel format. At this level of concentration, the priority is to preserve the chemical behavior of the acid and to maintain a predictable response during application. A liquid formulation supports this objective more reliably than a gel structure when high-strength TCA is involved.
In practical terms, this means that TCA 30% must be approached as a clinically controlled acid solution, not as a cosmetically thickened peel. The formulation itself reflects a professional philosophy: chemical precision first, texture second.
Liquid-only format aligned with high-strength acid stability requirements
Cleaner clinical handling when precise exposure timing is essential
No artificial thickening logic imposed on a concentration that demands chemical rigor
Better conceptual fit with advanced professional peeling strategies
Clinical formulation logic: above lower-strength presentation ranges, TCA is no longer merely a peel to spread — it becomes a controlled chemical intervention whose formulation must remain compatible with concentration, stability, and predictable tissue response.
Not a Gel by Design
Unlike lower concentrations that may tolerate broader presentation formats, TCA 30% is positioned here as a liquid acid only. This is not a missing feature. It is a deliberate scientific choice, since gel-based presentations above 18% are not considered chemically stable enough for a coherent high-strength TCA strategy.
Precision of Application
A liquid formulation allows the practitioner to work with controlled loading, defined contact, and disciplined distribution according to indication, skin zone, and endpoint strategy. At this concentration, application technique is part of the treatment itself.
Authority Through Chemical Coherence
Presenting TCA 30% as liquid only reinforces a medically coherent message: strong acids should not be reformulated for visual reassurance when their concentration demands respect, clarity, and technical expertise.
TCA 30% should therefore be understood not as a thicker or more convenient version of TCA, but as a high-strength acid formulation whose presentation follows the chemistry, not the marketing.
Purity, Concentration and Chemical Reality
The real strength of a TCA solution is not defined by the label alone. It depends on how concentration is expressed, how the solution is prepared, and how chemically coherent the formulation remains. Misinterpretations at this level lead directly to incorrect clinical expectations.
Beyond the “30%” Illusion
A true 30% w/w solution contains 30 g of trichloroacetic acid in 100 g of final solution. This is fundamentally different from simplified dilution practices frequently used in non-standard preparations.
A common shortcut consists in adding 30 g of TCA crystals to 100 ml of water. This produces a solution closer to 23% w/w, not 30%. It is often perceived as “30%” in practice, yet it does not represent the same chemical intensity.
True 30% w/w = 30 g / 100 g solution
Shortcut dilution:
30 g + 100 ml water → ≈ 23% w/w
Result: a true 30% w/w formulation is significantly stronger than most so-called “30%” preparations.
In addition, a 30% w/w solution corresponds approximately to a higher w/v equivalent (~35%), reinforcing the gap between nominal labeling and real chemical strength.
Material Compatibility & Storage
High-strength TCA must be stored in amber glass containers. This is not optional. Light exposure degrades the solution, and transparent packaging fails to provide adequate protection.
Plastic containers are incompatible with high-concentration acids. At this level of reactivity, interaction between the acid and the container material is not theoretical — it is expected. Any such interaction compromises chemical integrity and clinical predictability.
A serious formulation cannot rely on reactive storage systems. Glass remains the only coherent choice for maintaining stability in high-strength acid solutions.
Purity Is Not a Detail
At high concentration, even minimal contamination becomes clinically relevant. The presence of metallic ions or impurities can modify the chemical behavior of the solution and alter the biological response.
In some cases, this may lead to deep dermal staining rather than superficial hyperchromia. These pigment alterations behave more like chemical tattooing and are considerably more difficult to correct.
This is why high-purity TCA crystals and demineralized, bi-distilled water are not optional specifications, but essential requirements for a controlled medical-grade formulation.
Chemical Coherence Defines Clinical Outcome
A high-strength peel is not defined by its percentage alone, but by the coherence of its entire chemical system: concentration expression, purity, solvent quality, and storage conditions.
When these parameters are not respected, the practitioner is no longer working with a predictable chemical tool, but with an unstable approximation.
TCA 30% w/w must therefore be understood as a precise chemical intervention, not a nominal concentration label.
The difference between a nominal 30% solution and a true 30% w/w high-purity formulation is not theoretical. It is directly expressed in tissue response, depth control, and clinical outcome.
Understanding Frosting, Coagulation and Clinical Control
At 30% w/w, TCA is no longer a simple peeling agent. It becomes a controlled chemical coagulation system in which outcome depends on real-time interpretation of tissue response. The practitioner must evaluate frosting dynamics, anatomical resistance, pressure modulation, and exposure control rather than relying on concentration alone.
Frosting Patterns as Biological Endpoints
Frosting should never be interpreted as a decorative surface effect or as mere “coverage.” It reflects progressive protein coagulation and provides a visual endpoint that helps guide the depth and intensity of the chemical reaction during TCA application.
Progressive frosting patterns during TCA application, from superficial epidermal coagulation to dense protein coagulation. These visual stages help the practitioner assess the biological response rather than simply the apparent whiteness of the surface.
Application Dynamics and Penetration Control
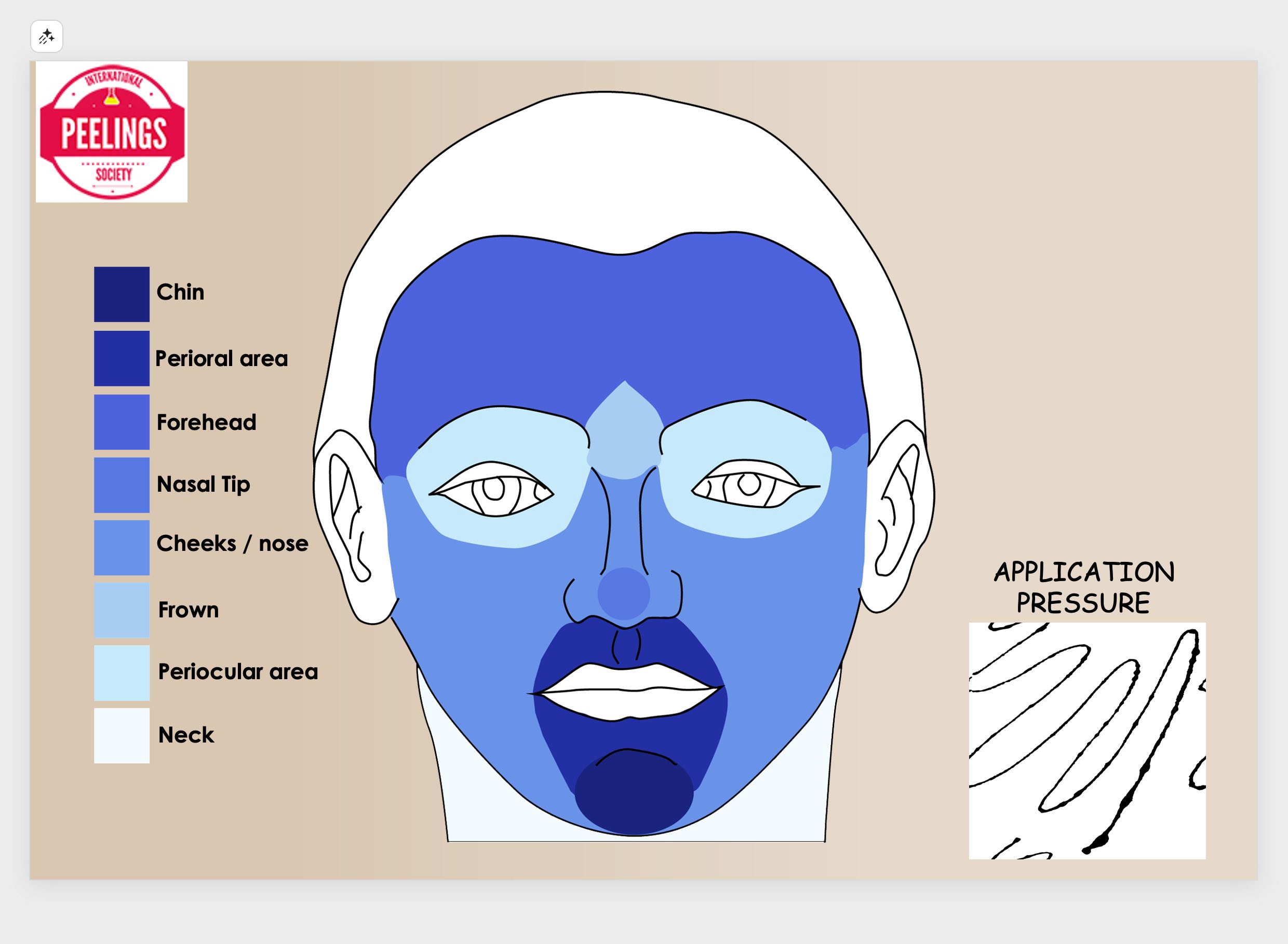
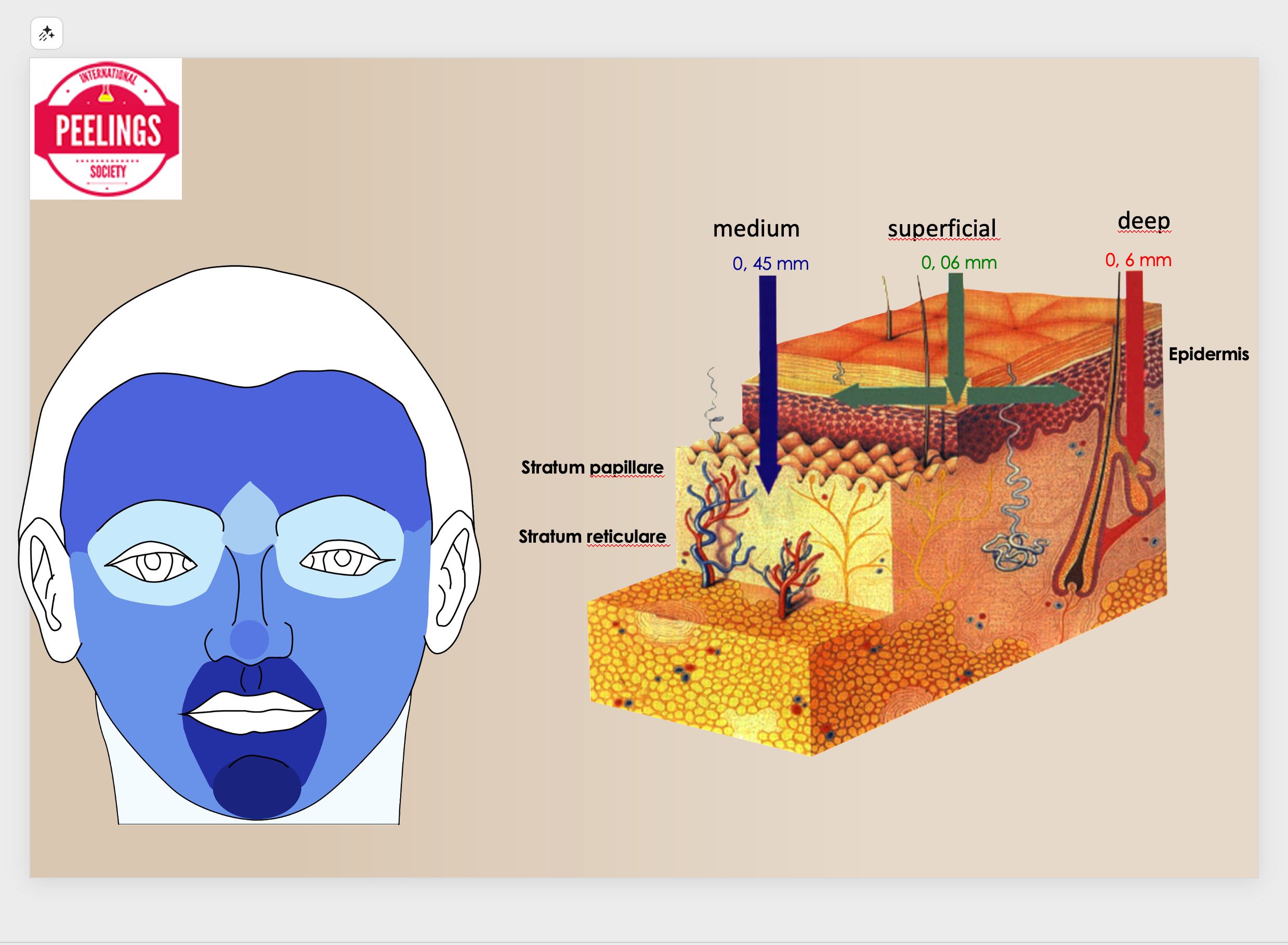
Penetration depth is not defined by concentration alone. According to the application model associated with Mauro Tiziani, pressure, anatomical zone, skin resistance, and operator technique directly influence TCA diffusion and coagulation behavior. TCA 30% must therefore be considered a dynamic physician-controlled tool, not a static percentage.
Facial pressure modulation influences acid behavior differently across anatomical zones. Thin and reactive areas require lighter application, while thicker zones may tolerate a more controlled mechanical engagement.
The observed endpoint depends on how the chemical reaction interacts with epidermal and dermal structures. Clinical depth is engineered through application strategy, not estimated from concentration alone.
Penetration depth and clinical outcome are determined by application control, pressure distribution, anatomical variability, contact time, and observed tissue response.
Concept adapted from Mauro Tiziani and integrated here into an advanced TCA 30% application framework.
Frosting Is a Biological Endpoint
Frosting represents protein coagulation, not simple product deposition. Its intensity reflects a biological reaction within the tissue and must be interpreted in relation to indication, skin thickness, and evolving clinical response.
Depth Is Not Defined by Layers Alone
Multiple passes do not automatically produce safer or more effective penetration. Depth is influenced by concentration, pressure, contact time, epidermal resistance, and anatomical variability. Uncontrolled layering only increases risk.
Timing Is a Major Control Variable
At 30%, exposure time becomes a decisive parameter. A delayed interruption of the reaction or excessive contact may convert a controlled endpoint into an unpredictable injury pattern. Precision in timing is therefore essential.
Application Technique Defines Outcome
Pressure, saturation, movement, and distribution pattern directly influence how TCA interacts with the skin. TCA 30% requires disciplined operator control rather than uniform spreading or routine layering.
Observed Reaction Prevails Over Nominal Percentage
Clinical decisions must be guided by the actual tissue response. A well-controlled TCA 30% application may be more predictable than a poorly executed lower concentration used without biological interpretation.
Controlled Injury Supports Regeneration
The objective is not aggressive destruction but a controlled coagulative stimulus capable of initiating a regenerative response. Excessive force, poor timing, or misread endpoints increase complications rather than efficacy.
⚠️ TCA 30% requires real-time clinical judgment. There is no universal application pattern suitable for every indication. Technique must be adapted to the treatment objective, anatomical site, skin behavior, and immediate coagulation endpoint observed during the procedure.
Mastery of TCA 30% does not come from concentration knowledge alone. It depends on the practitioner’s ability to interpret frosting, control penetration, and modulate the chemical reaction as it unfolds in real time.
Clinical Use Cases & Strategic Superiority
TCA 30% is not a universal peel for every scenario. Its true value appears in selected clinical contexts where controlled coagulation, precise lesion coverage, and operator-driven depth modulation provide a strategic advantage over more superficial approaches.
TCA 30% becomes strategically superior when superficial approaches fail, when homogeneous lesion coverage is clinically required, and when the practitioner is able to interpret coagulation endpoints in real time. It should not be viewed as merely a stronger peel, but as a more exact and more operator-dependent instrument.
Combination Strategies & Clinical Modulation
TCA 30% should not be used as an isolated intervention. Its full clinical potential emerges when combined with complementary agents that modulate penetration, control coagulation, and optimize tissue recovery.
Clinical Control
Frosting Control & Delimitation
Peeling de Luxe Plus can be applied to interrupt and control the progression of frosting, allowing precise delimitation of treated areas and preventing unwanted diffusion.
Strategic role: supports controlled endpoint management during advanced pigment-oriented application.
Aseptiskin ensures optimal skin preparation without altering surface markings, preserving accuracy of application and improving homogeneity of the chemical response.
Strategic role: improves procedural precision before TCA contact with the skin.
Lipoic Acid can be integrated to modulate penetration depth and reduce excessive coagulation in sensitive areas, improving control over clinical outcomes.
Strategic role: helps refine reactivity in more delicate zones or adjusted protocols.
The effectiveness of TCA 30% lies not only in its concentration, but in the practitioner’s ability to integrate it into a broader therapeutic strategy. Combination protocols transform TCA from a chemical agent into a controlled clinical system.
Clinical Questions on TCA 30%
The following points address common clinical misunderstandings and practical questions related to the use of TCA 30%. This section is intended for trained practitioners familiar with chemical peeling techniques.
Is TCA 30% considered a deep peel?
Not necessarily. Depth is not defined by concentration alone. Depending on application technique, pressure, and contact time, TCA 30% may act at superficial or medium levels. The observed endpoint (frosting) is more relevant than nominal percentage.
Does more layers mean deeper penetration?
No. Multiple passes without control do not ensure deeper or better outcomes. Penetration is governed by tissue response, exposure time, and operator technique. Excess layering increases risk rather than efficacy.
How should frosting be interpreted clinically?
Frosting reflects protein coagulation and should be interpreted as a biological endpoint, not as a visual target. Its intensity and distribution must be correlated with anatomical area, indication, and real-time tissue response.
Is TCA 30% suitable for melasma?
Yes, when applied with strict control. TCA 30% allows homogeneous coverage of the pigmented area, but requires precise delimitation and appropriate combination strategies to avoid irregular outcomes or demarcation lines.
Can TCA 30% be used on all skin types?
It can be used across different phototypes, but requires careful adaptation. Higher phototypes demand increased control, precise application, and appropriate pre- and post-treatment management to reduce risk of dyschromia.
Why combine TCA 30% with other agents?
Combination strategies allow modulation of penetration, control of frosting progression, and optimization of recovery. TCA should be considered part of a broader clinical system rather than a standalone intervention.
Is TCA 30% safe without experience?
No. TCA 30% requires real-time clinical judgment and understanding of skin response. It is not recommended for inexperienced users or non-medical settings.
This information is intended for trained professionals. Proper indication, technique, and clinical judgment are essential for safe and effective use of TCA 30%.
For Professional Use
Bring TCA 30% Into a Controlled Clinical Strategy
TCA 30% should not be approached as a simple percentage, but as a physician-controlled coagulation instrument. When paired with proper preparation, endpoint interpretation, and combination support, it becomes a highly strategic tool for advanced pigment, texture, and resurfacing protocols.
Advanced Clinical PositioningDesigned for practitioners who require endpoint-driven control rather than routine superficial peeling.
Protocol-Based UseIntegrates naturally into structured treatment pathways, not isolated one-step procedures.
Combination-Ready SystemCan be modulated with preparation, delimitation, recovery, and support products when clinically indicated.
Professional Knowledge RequiredBest results depend on application discipline, anatomical judgment, and real-time interpretation.
Choose Your Next Step
Whether your priority is immediate product access, a deeper understanding of indication-based protocols, a paid teleconsultation, or hands-on training, the next step should remain clinical, structured, and professionally guided.
This page was built to support clinical decision-making, not impulse use. It helps practitioners understand where TCA 30% becomes relevant, how it should be controlled, and why strategic combinations matter.
Need product access?Use the professional login to reach restricted medical product access reserved for qualified practitioners.
Need protocol guidance?Review the relevant clinical protocol pathways before selecting indication-specific use.
Need direct support or practical training?Choose a paid teleconsultation for focused guidance or join a hands-on workshop for procedural training.
TCA 30% is intended for trained professionals able to evaluate skin behavior, endpoint progression, and indication-specific risk. Clinical judgment remains essential at every stage of application.
Strategic Clinical Summary
TCA 30% should be interpreted as a controllable coagulation system rather than a predefined-depth peel. Its clinical value lies in the practitioner’s ability to modulate application parameters, interpret frosting dynamics, and adapt penetration to indication-specific objectives.
When integrated into structured protocols and supported by appropriate combination strategies, TCA 30% enables targeted lesion coverage, refined modulation of pigmentation and texture, and reproducible biological responses across different clinical contexts.
In this perspective, TCA 30% is not defined by its concentration, but by the precision of its use — requiring disciplined technique, endpoint control, and clinical judgment.