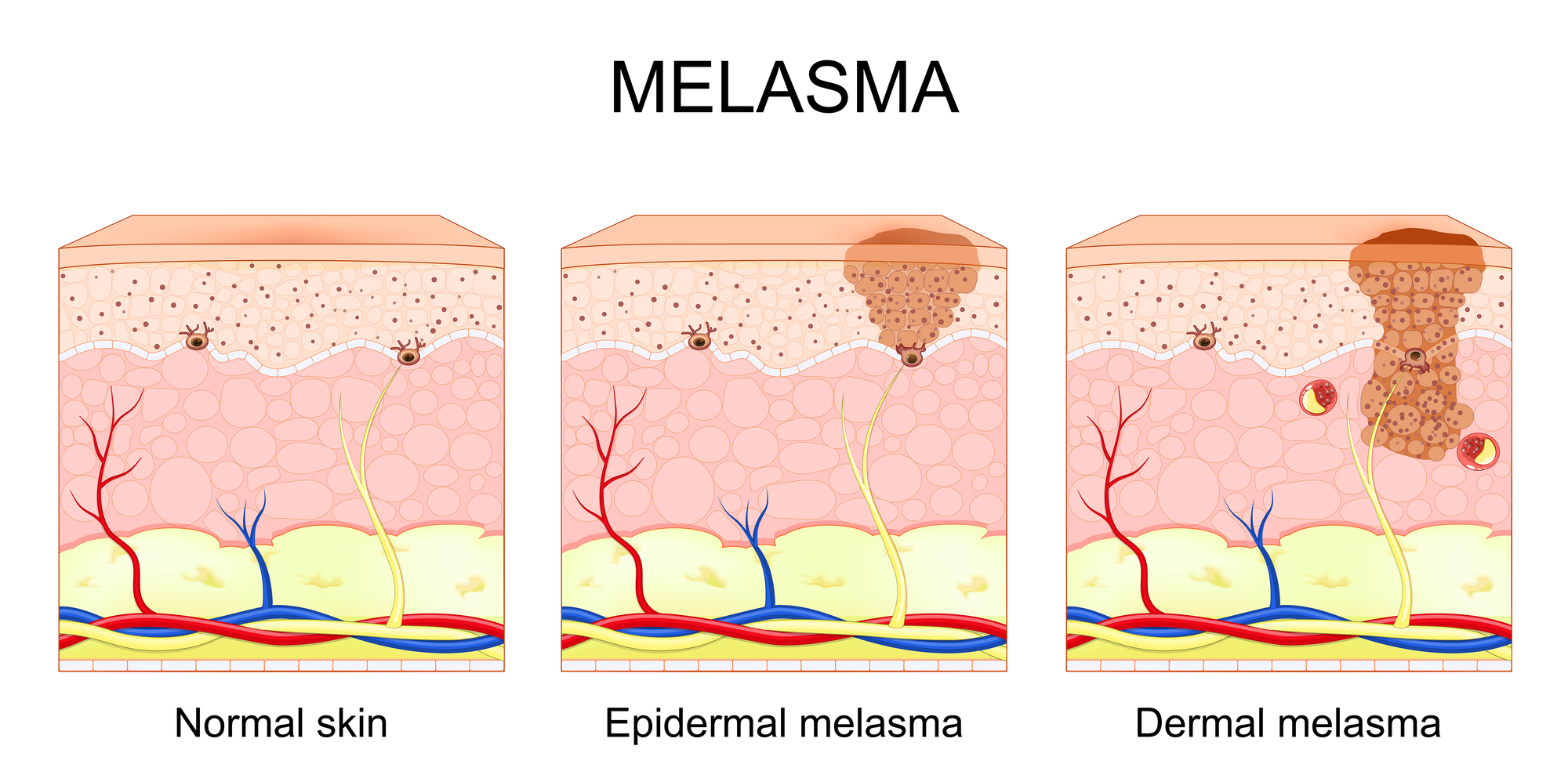
In melasma, acid selection should not be reduced to concentration alone. Once pigment dysregulation has become clinically established, the functional behavior of acids must be interpreted according to their biologic endpoint, corrective role, and capacity to stabilize the epidermal environment over time.
In melasma, lower pKa acids are more relevant when a stronger corrective endpoint is required, intermediate pKa acids are useful for regulatory transition and controlled epidermal renewal, while higher pKa systems may support stabilization, tolerance, and long-term maintenance. The objective is not random exfoliation, but biologically guided pigment control.
Low pKa • < 2
Direct Corrective Activity &
Pigment Reduction
Lower pKa acids are associated with stronger immediate biologic activity and may be more relevant when visible corrective action is intended in pigment-loaded epidermal zones.
- More suitable for stronger corrective endpoints
- Relevant when visible pigment reduction is required
- Must be interpreted in relation to phototype and tolerance
Intermediate pKa • 2–4
Keratoregulation &
Progressive Modulation
Intermediate pKa acids often provide a bridge between activity and tolerance, supporting progressive epidermal renewal and biologically regulated pigment management.
- Useful in transitional corrective strategies
- Supports controlled epidermal turnover
- Relevant for sequential and combined protocols
Higher pKa • > 4
Stabilization Without
Excessive Irritative Load
Higher pKa systems are more appropriate when the clinical priority is support, tolerance, epidermal balance, and long-term stabilization of dyschromic skin behavior.
- Supports maintenance and epidermal comfort
- Useful in sensitive or reactive cutaneous environments
- Relevant for maintenance after corrective phases
1
Prepare
Optimize the epidermal environment with better tolerated systems before introducing stronger corrective strategies in unstable pigment disorders.
2
Correct
Use more active corrective acids only when the clinical endpoint, phototype, and biologic context justify a stronger intervention.
3
Stabilize
Maintain gains through progressive support, tolerance-oriented management, and reduction of relapse toward recurrent pigment expression.
Scientific Blocks for Clinical Interpretation
Pigment Objective
The aim is not merely to exfoliate, but to reduce visible dyschromia while respecting the biologic behavior of melasma-prone skin.
Biologic Principle
Regulated progression is preferable to uncontrolled irritative excess. The most effective strategy is usually sequential, not indiscriminate.
Clinical Caution
Phototype, epidermal instability, topical environment, and relapse tendency must guide every therapeutic decision in melasma management.